While in children with facial palsy the eye closure function often suffices for years or decades to wet the cornea, the protection of the cornea of the eye has top priority in adults. In addition to conservative measures such as instilling artificial tears and applying "watch glass bandages" at night, it is advisable in adults to apply a small gold/platinum weight to the upper eyelid at a hidden point during the first weeks after the onset of facial paralysis in order to prevent permanent damage. This can help the patient to restore an approximate eye closure and a physiologically important blinking reflex for corneal wetting. This successfully averts an impending corneal damage with insufficient wetting with tear fluid.
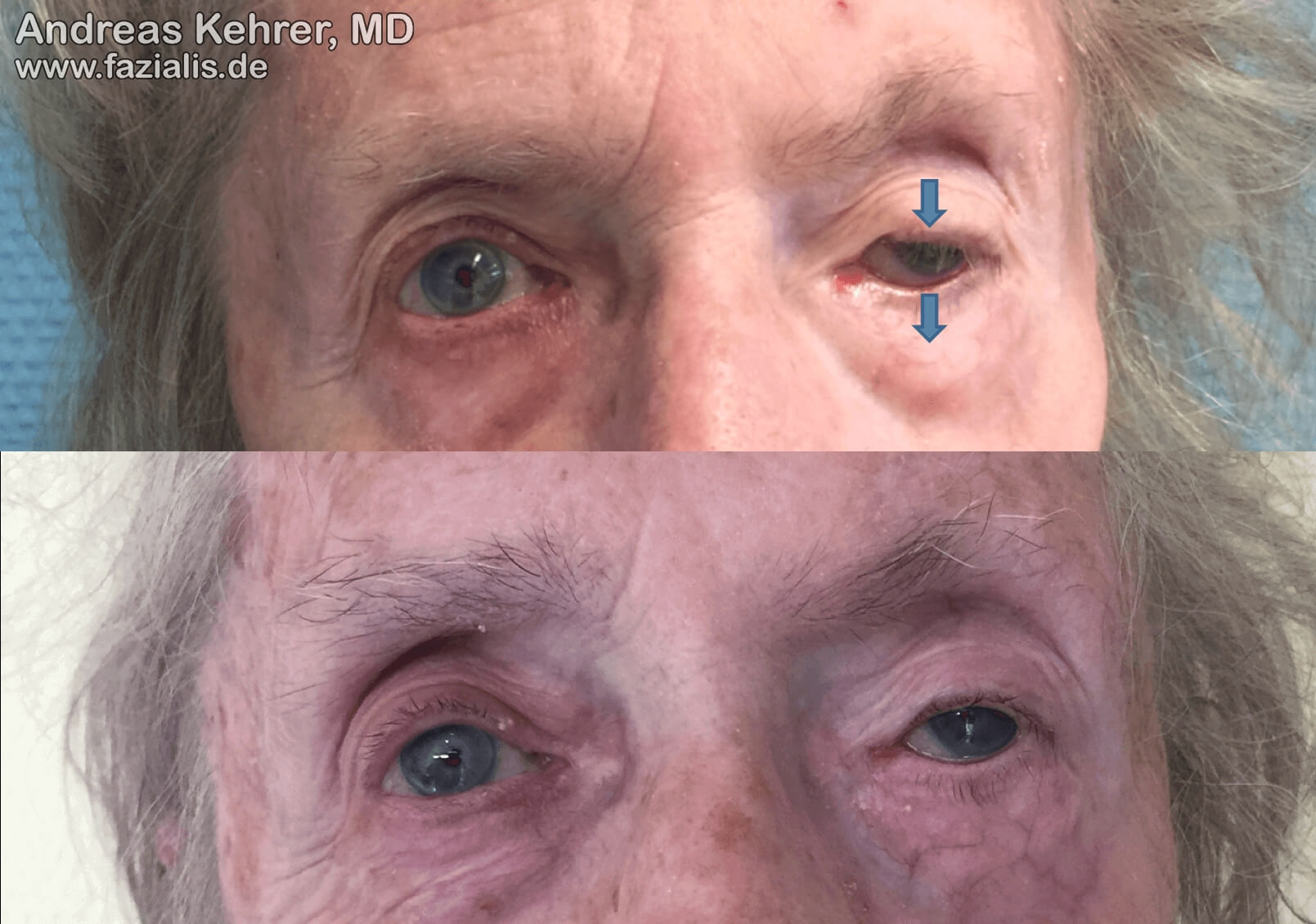
The gold and platinum implants used to weigh the upper eyelids are very small. We prefer a very modern technique of insertion, which avoids visibility of the implant under the upper lid skin. While in the older lady the contours of the somewhat too heavy implant are visible directly under the skin (external operation) in the upper picture, after the insertion of a minimally lighter implant this is no longer perceptible due to the new technique. The corrected position of the upper eyelid no longer covers the pupil and allows the patient to see in this eye.


An even clearer difference becomes apparent when closing the eyes. The lady is now impressed by the elongated weight with clearly visible projection under the thin skin of the upper eyelid. It seems a little too lightly chosen. In some older patients the standard technique of placement leads to a slowly increasing skin atrophy, which can lead to an exposure of the weight and finally to an implant infection. In these cases, the weight must be removed. In the young patient in the right picture, the platinum weight is still not noticeable even when the eye is completely closed. Nevertheless, a complete eye closure is possible with the help of the weight. The fine incision is placed directly into the natural upper eyelid crease so that no visible scar remains. The special positioning also means that the weight is no longer perceived as disturbing by the patient. It is no longer perceptible to them after healing. If the implants are really not tolerated by the patient, they can be easily removed again without any secondary damage. This can also be done if the implant is only used as a bridging measure until the nerve control of the eye sphincter (m. orbicularis oculi) has been regenerated by surgery or spontaneous healing.

An even clearer difference becomes apparent when closing the eyes. The lady is now impressed by the elongated weight with clearly visible projection under the thin skin of the upper eyelid. It seems a little too lightly chosen. In some older patients the standard technique of placement leads to a slowly increasing skin atrophy, which can lead to an exposure of the weight and finally to an implant infection. In these cases, the weight must be removed. In the young patient in the right picture, the platinum weight is still not noticeable even when the eye is completely closed. Nevertheless, a complete eye closure is possible with the help of the weight. The fine incision is placed directly into the natural upper eyelid crease so that no visible scar remains. The special positioning also means that the weight is no longer perceived as disturbing by the patient. It is no longer perceptible to them after healing. If the implants are really not tolerated by the patient, they can be easily removed again without any secondary damage. This can also be done if the implant is only used as a bridging measure until the nerve control of the eye sphincter (m. orbicularis oculi) has been regenerated by surgery or spontaneous healing.

External weights for lid-loading of the upper eyelid, which are fixed with a skin adhesive or with a double-sided adhesive strip, are aesthetically quite compromising. They have the same functional effect as the implantable weights and support eyelid closure in an upright body position. Although they are not a permanent solution for most patients, they can be a useful temporary measure for corneal protection.

Eye bubble moisture chambers, as seen here in the middle picture, are effective in the short term to protect the cornea from drying out. However, they are often only an auxiliary, quite costly and bridging measure during the day. They do not restore eyelid closure. The insertion of a small platinum weight (right picture) is very well tolerated by the patients and is not perceived as disturbing ("you don't feel it at all"). They result in better eyelid closure in everyday life. Should the function of the facial nerve and thus active eyelid closure be restored in the course of reinnveration, it can be removed again without any problems via the same invisible skin incision on the upper eyelid.
