Prognosis of spontaneous, idiopathic facial paralysis (Bell paresis)
Prognosis of facial palsy: most cases of spontaneous facial paralysis resolve on their own. In 71% of the cases, no consequential damage remains; 84% of the patients regain an almost normal function[1,2]. However, the remaining patients often suffer considerably from the loss of the facial nerve. The reduced function often includes muscular weakness of the facial musculature, synkinesis (unwanted mass movements), or muscle spasticity. Facial pain, the cause of which has not yet been fully clarified, has also been described[3,4].
The severity of of facial paralysis at first onset is of crucial prognostic importance. In a recent scientific study by Fujiwara et. al on a large series of patients, it was described that the sole prognostic factor was the extent of functional failure one week after first onset[5]. This means that the more serious the symptoms are one week after the occurrence of Bell's palsy, the worse the worse prognosis is for the expected recovery of function.
This was confirmed in the large reference studies by Peitersen et. al.[1, 2]. If only partial paralysis occurred at the beginning of Bell's palsy, 94% of the patients in his study showed a complete regression of paralysis within four months. However, if there was complete facial paralysis from the beginning, only 61% of the patients showed a complete regression of symptoms during the course of the study. 39% of the patientssuffered from permanent loss of function.
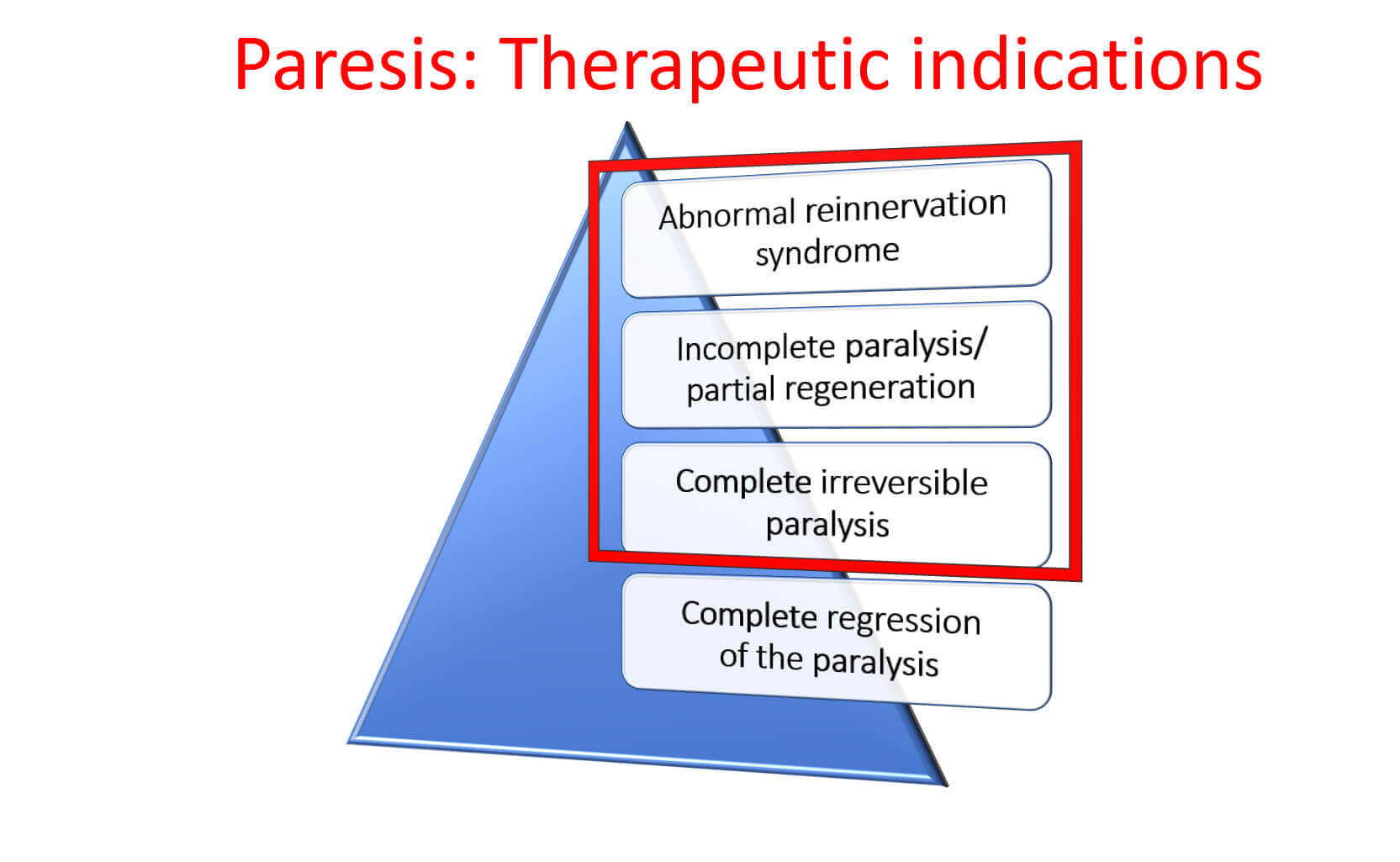
According to an observational study in untreated patients, in 85% of the cases there was a regression within 3 weeks after the onset of symptoms and in 10% a partial regression after 3-6 months. In 71% of the cases, the regression is complete; in 13% incomplete, but without significantly affecting the patient . In 16% of the patients, the reinnervation is so aberrant that synkinesis, autonomous disorders (crocodile tears), and/or contractures occur[1,6].
In a follow-up study with a 34% share of non-idiopathic facial nerve palsies, 71% experienced complete regression, 12% mild residual symptoms, 13% mild dysfunction, and 4% severe residual dysfunction (Peitersen, 2002). Favorable prognosis can also be seen from the data of the placebo groups in the two most recent large therapy studies. After 3 and 9 months, 65% and 85% of placebo-treated patients, respectively, showed complete remission in the study conducted by Sullivan (Sullivan et al., 2007) and 65% of placebo-treated patients in the Engström-led study (Engström et al., 2008) after 12 months. In general, patients with incomplete paresis showed a better tendency to recover (94%) (Ronthal, 2016). Facial nerve palsies after zoster infection more often lead to incomplete recovery. Borrelia-induced facial nerve palsies almost always have a good prognosis (Angerer et al., 1993).
Sources:
[1] Peitersen E. The natural history of Bell’spalsy. Am J Otol 1982;4:107–11.
[2] Peitersen, E. Bell’s Palsy: The Spontaneous Course of 2,500 Peripheral Facial Nerve Palsies of Different Etiologies. Acta Otolaryngol 2002; Suppl 549: 4–30
[3] Holland NJ, Weiner GM. Recent developments in Bell’s palsy. Br Med J 2004;329:553–7.
[4] Morgenlander JC, Massey EW. Bell’s palsy. Ensuring the best possible outcome. Postgrad Med 1990;88:157–61, 164.
[5] Fujiwara T, Hato N, Gyo K, et al. Prognostic factors of Bell’s palsy: prospective patient collected observational study. Eur Arch Otorhinolaryngol (2014) 271:1891–1895
[6] S2-Leitlinie "Therapie der idopathischen Gesichtlähmung (Bell's Palsy)" der Deutschen Gesellschaft für Neurologie (DGN) März 2017: www.awmf.org/leitlinien/detail/ll/030-013.html
[7] Boahene K, Facial reanimation after acoustic neuroma resection: options and timing of intervention. Facial Plast Surg. 2015 Apr;31(2):103-9