Additional corrective options such as botulinum toxin injection (e.g. for hyperactive muscle groups, also called "hemispasm facialis" or "blepharospasm"), and fat transfers ("lipofilling” or “lipografting") for the correction of volume deficits in the face are part of the range of procedures. Synkinesis (abnormal unwanted facial expressions, unintentional twitches) and muscular hardening (spasticity) can be treated by selective surgical nerve separation (partial separation of nerve branches under the microscope) or with botulinum toxin ("Botox“).
The mechanism of action of botulinum toxin consists of the enzymatic degradation of presynaptic proteins of the nerve endings at the motor end plates, which are required for the docking of synaptic vesicles to the presynaptic membrane. In the absence of transmitter release from the endings of the facial nerve, the muscles innervated by the facial nerve are functionally denervated; they can no longer contract.
Botulinum toxin, a toxin produced by the bacteria Clostridia, works by blocking the release of the messenger substance acetylcholine from the nerve endings. With subcutaneous injections, this effect begins after a few hours, a full effect is achieved after one to two weeks. The motor end plates are removed, but after weeks or months new end plates are formed, which form functional neuromuscular transfer sites with newly sprouted nerve endings.

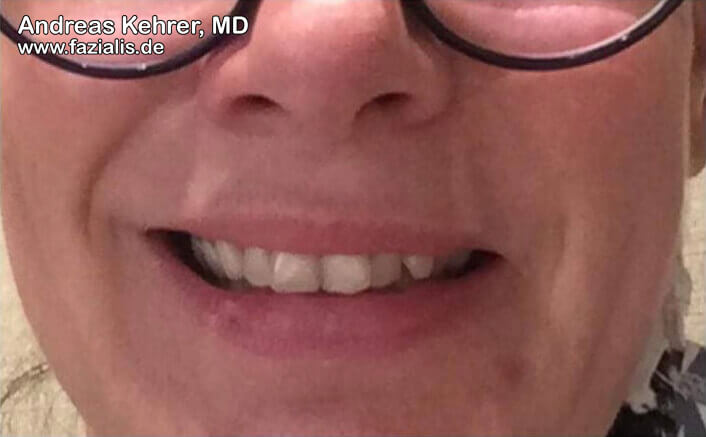
46-year-old patient with a spastic form of facial nerve palsy with clear synkinesias on the left side. When smiling, the mouth angle-lowering musculature on the left is so hyperactive that a smile on the side is literally suppressed (see the pit at the bottom of the left picture). When smiling, the eye ring muscle on the left side is unintentionally overactivated, which leads to a conspicuously small cleft eyelid. Finely dosed amounts of botulinum toxin were a good remedy: the right picture shows a much more harmonious smile, the left corner of the mouth "points upwards". At the same time, the blepharospasm (involuntary cramping of the eye ring muscle) in the left eye has vanished: this results in a considerably improved overall symmetry of the smile. This significantly improves the patient's social function.
The toxin is injected at four to six points above the upper and lower part of the orbicularis oculi muscle (eye ring muscle). If the zygomaticus major muscle is also activated in the spasms, an additional injection into the nasolabial fold can be performed.
It is not uncommon for the spasms in the uninjected orbicularis oris muscle to improve, which is usually omitted by the injection due to the danger of facial asymmetry even at small doses.
The partial functional denervation of the mimetic musculature causes a considerable to complete regression of the facial hemispasm. Clinically, the denervation often recedes completely; after about three to six months, involuntary contractions occur again. Then a new injection is necessary.
As a side effect of the therapy, there may be a weakness of the mimic musculature which is stronger and more extensive than desired. The weakness of the M. levator palpebrae superioris most frequently occurs with the development of a partial ptosis (hanging upper eyelid). Like the desired therapeutic effect, muscle weakness, which may occur as a side effect, is temporary and subsides after a few weeks.