A widespread and recognized classification for the extent of facial nerve palsy is the classification established in 1985 according to House and Brackmann.[1] The so-called "Facial Nerve Grading System" according to John House and Derald Brackmann divides the severity of the resulting immobility of the mimic musculature into six degrees:
Grading of facial savings according to House-Brackmann
| Degree | Function | Repose | Front | Lid Closure | Mouth |
|---|---|---|---|---|---|
| I: normal | normal | normal | normal | normal | normal |
| II: slight paresis | weakness/synkinesia, only recognizable on close observation | normal | reduced | fast normal | low |
| III: moderate paresis | obvious lateral difference, synkinesia, contracture | normal | not present | complete | small reduced |
| IV: moderately strong paresis | adjusting asymmetry | normal | no | incomplete | asymmetry |
| V: strong paresis | No residual mobility detectable | Asymmetry | No | Incomplete | Asymmetry |
| VI: Paralysis | No residual mobility visible | Tone loss | None | None | None |
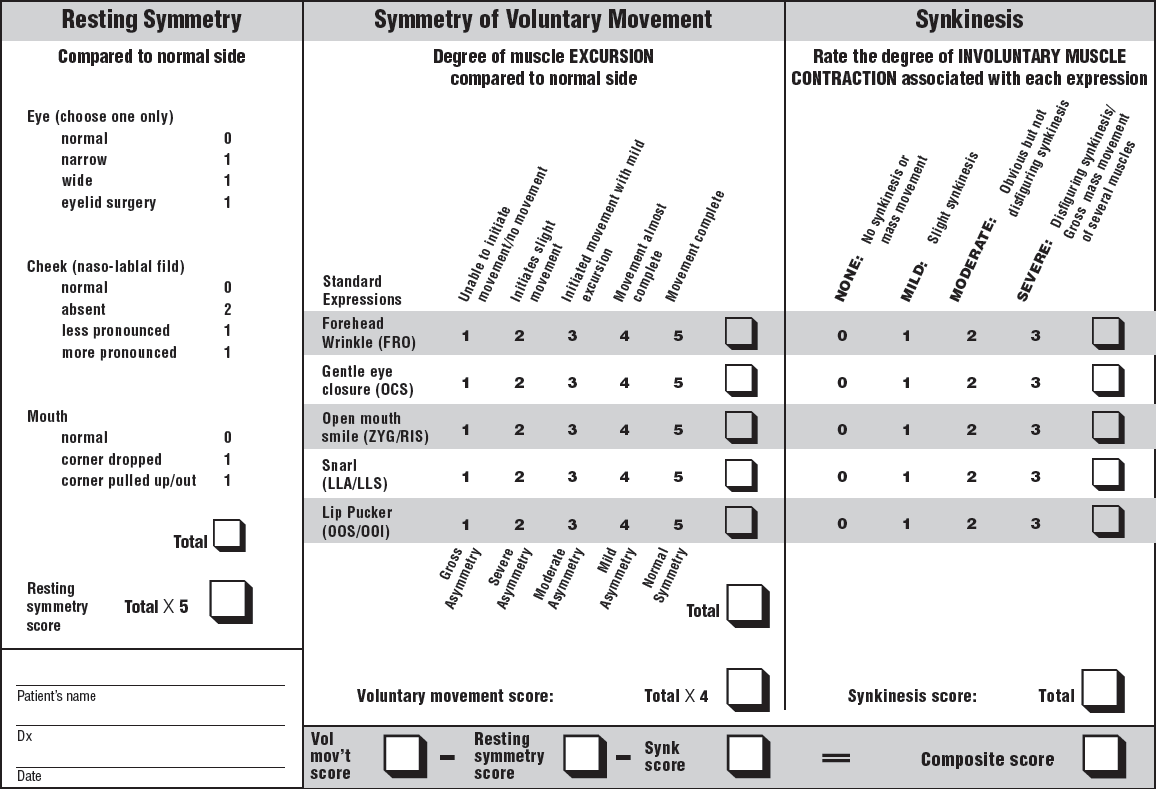
Furthermore, the "Sunnybrook Facial Grading System" according to Brenda Ross et al., which originates from Toronto (Canada), has established.[2] In this test method, which was presented in 1992, local parameters are examined. Originally developed to measure the healing process after removal (resection) of auditory nerve tumors (vestibularis schwannomas),[3] it offers a recognized diagnostic tool due to its high sensitivity and reliability.[4,5,6] Resting symmetry, symmetry in motion and synkinesis are evaluated according to the following schemes
Both the Sunnybrook Facial Grading Score and the House Brackmann Score are well established in clinical routine. In addition, there is a large number of other classification systems, which will be illustrated by example. The Burres and Fish classification from 1986 represents an objective distance measurement between landmarks on the face.[7] The measured values are taken at rest and when five different facial expressions are executed. A disadvantage is the difficult handling. A simplified version of the method according to Burres and Fisch is the Nottingham System. Here, the measurement of four aspects takes place in three different facial poses. The paralyzed side is compared with the healthy side. As a consequence, the Nottingham Score is not applicable in bilateral facial nerve palsies.[8]
In 1987, Chevalier et al. developed a five-step scale.[9] Here, a value of 0 equates to no contraction, while a value of 4 requires synchronous and symmetrical movement of the two halves of the face. However, a separate evaluation of facial regions is not possible.
The Yanagihara system is used especially in Japan.[10] The classification is based on the subjective evaluation of ten different facial expressions. The classification is carried out by the treating physician and is thus person-dependent. Furthermore, any consequences of facial nerve palsy are not included in the evaluation.
An interesting approach is the program "eFACE", which was developed in 2015 by Tessa and Charles Hadlock, Phrabat Bhama, Charoline Banks and Jong Park.[11] Based on 16 test values (items) in the format of a visual analogue scale (see Fig. 1), facial functions and symmetry can be mapped. The use of eFACE is initially limited to unilateral facial nerve palsies.

Source: Wagner A, Blunk J, Benrath J. Neuropathic and tumor-related headache. ENT 59,2011; 656-663. doi.org/10.1007/s00106-011-2269-0.
Sources:
[01] House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985;93(2):146–7. PubMed PMID: 3921901.
[02] Ross BG, Fradet G, Nedzelski JM. Development of a sensitive clinical facial grading system. Otolaryngol Head Neck Surg. 1996;114(3):380–6. PubMed PMID: 8649870.
[03] Banks CA, Bhama PK, Park J, Hadlock CR, Hadlock TA. Clinician-Graded Electronic Facial Paralysis Assessment: The eFACE. Plast Reconstr Surg. 2015 Aug;136(2):223e-230e. doi: 10.1097/PRS.0000000000001447. PMID: 26218397.
[04] Ahrens A, Skarada D, Wallace M, Cheung JY, Neely JG. Rapid simultaneous comparison system for subjective grading scales grading scales for facial paralysis. Am J Otol. 1999;20(5):667–71. PubMed PMID: 10503592.
[05] Kayhan FT, Zurakowski D, Rauch SD. Toronto Facial Grading System: interobserver reliability. Otolaryngol Head Neck Surg. 2000;122(2):212–5. doi: 10.1016/S0194-5998(00)70241-5. PubMed PMID: 10652392.
[06] Hee GH, Nedzelski JM. Facial nerve grading systems. Facial Plast Surg. 2000;16(4):315–24. doi: 10.1055/s-2000-15547. PubMed PMID: 11460297.
[07] Burres S, Fisch U: The comparison of facial grading system. Arch Otolar- yngol Head Neck Surg, 1986, 112: 755–758.
[08] Kang TS, Vrabec JT, Giddings N, et al.: Facial nerve grading systems (1985–2002): beyond the house- Brackmann scale. Otol Neurotol, 2002, 23: 767–771.
[09] Fonseca KM, Mourão AM, Motta AR, Vicente LC. Scales of degree of facial paralysis: analysis of agreement. Braz J Otorhinolaryngol. 2015 May-Jun;81(3):288-93. doi: 10.1016/j.bjorl.2014.04.005. Epub 2014 Oct 18. PMID: 25497850.
[10] Berg T, Jonsson L, Engström M: Agreement between the Sunnybrook, House- Brackmann, and Yanagihara facial nerve grading systems in Bell’s palsy. Otol Neurotol, 2004, 25: 1020–1026.
[11] Banks CA, Bhama PK, Park J, Hadlock CR, Hadlock TA. Clinician-Graded Electronic Facial Paralysis Assessment: The eFACE. Plast Reconstr Surg. 2015 Aug;136(2):223e-230e. doi: 10.1097/PRS.0000000000001447. PMID: 26218397.