Time of treatment and operation
The timing of the therapy is of critical importance. It is still misunderstood by many medical colleagues, therapists and patients.
The best results are achieved with early treatment of facial paralysis.
OPHTHALMIC CONSIDERATIONS
Unlike in children with facial palsy where eye closure function often suffices for years or decades to wet the cornea, corneal protection is an urgent priority in adults. In addition to conservative measures, such as instilling artificial tears and applying "watch glass bandages" at night, it is advisable to apply a small gold/platinum weight to the upper eyelid at a hidden point during the first few weeks after the onset of facial paralysis in order to prevent permanent damage. This can help the patient to achieve at least an almost complete eye closure. This successfully averts an impending corneal damage with insufficient wetting with tear fluid.
OPERATIVE TIMING
For clinical practice, it is also important that after onset of facial nerve palsy and missing signs of an adequate functional restitution by nerve healing, plastic surgery should be started as early as 6 months to preserve the mimic musculature.
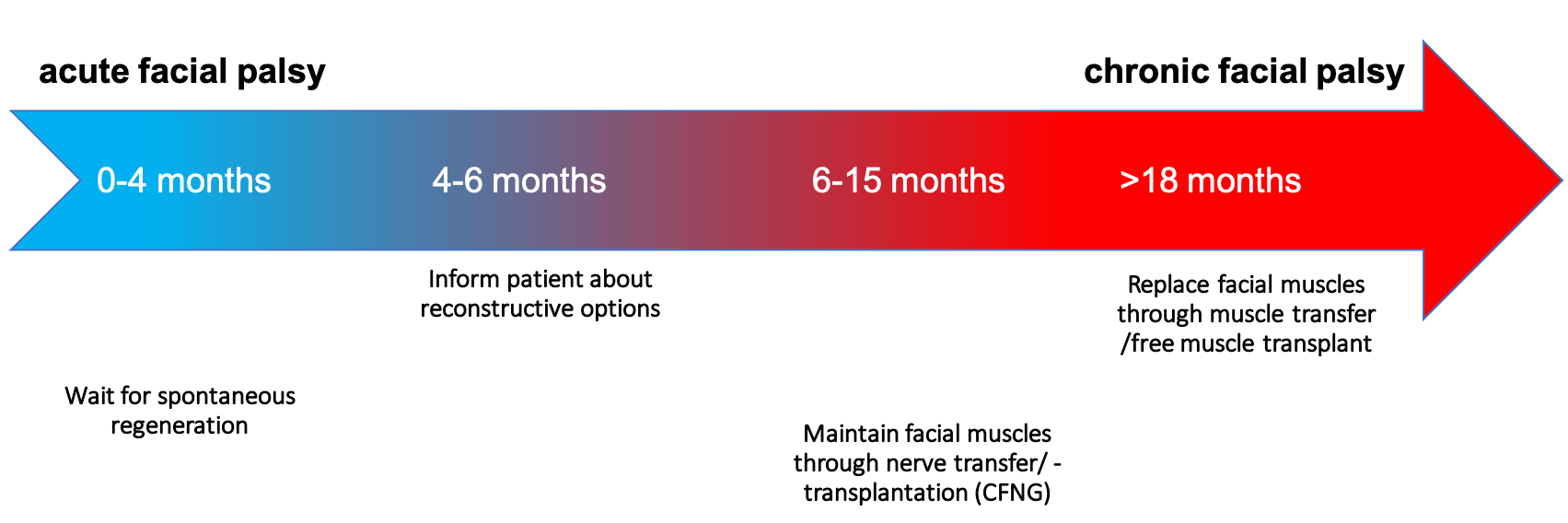
The "time-is-muscle" principle applies, because after a period of 15 to 18 months without using the mimetic muscles, these are irrevocably weakened due to the lack of nerve stimulation. The affected muscle groups are transformed into fatty tissue with a complete loss of facial expression and other important functions of the facial muscles. If, however, a nerve transfer and, if necessary, an additional nerve transplantation are performed before this point in time, the mimetic muscles can also be preserved without functioning facial nerves on the paralyzed half of the face and their original, detailed function may be able to be restored.
However, even after this time window has elapsed, there are still many possibilities. If nerve transfer is no longer possible, patients can be helped to achieve much more symmetry and dynamic function (movement, ability to react) of the face by introducing their own tissue, carrying out motor replacement plastic surgery (e.g. rearrangement of part of the masticatory muscles without loss of chewing ability) or free functional muscle transfer.


Sources:
[1] Biglioli F, Facial reanimations: part I--recent paralyses. J Oral Maxillofac Surg. 2015 Dec;53(10):901-6.
[2] Boahene K Reanimation of the paralyzed face F1000 Prime Reports 2013
[3] Yoshioka N, Masseteric nerve transfer for short term facial paralysis following skull base surgery, Journal of Plastic, Reconstructive & Aesthetic Surgery 2015
[4] Rivas A, A model for early prediction of facial nerve recovery after vestibular schwannoma surgery. Otol Neurotol 2011, 32:826-33
[5] Boahene K, Facial reanimation after acoustic neuroma resection: options and timing of intervention. Facial Plast Surg. 2015 Apr;31(2):103-9
[6] Albathi M, Early Nerve Grafting for Facial Paralysis After Cerebellopontine Angle Tumor Resection With Preserved Facial Nerve Continuity. JAMA Facial Plast Surg 2016
[7] Ray W, Motor Nerve Transfers: A Comprehensive Review, Neurosurgery 78:1–26, 2016
[8] Garcia R, Contemporary Solutions for the Treatment of Facial Nerve Paralysis, PRS 2015
[9] Eviston TJ, Croxson GR, Kennedy PGE, et al. Bell ’ s palsy : aetiology , clinical features and multidisciplinary care. 2015:1356-1361. doi:10.1136/jnnp-2014-309563.
[10] Özmen Ö,Outcomes of Facial Nerve Grafting in 155 Cases: Predictive Value of History and Preoperative Function, Otology & Neurotology, Vol. 32, No. 8, 2011