If the injured facial nerve does not heal after 1 to 1.5 years, or if the nerve is not surgically repaired within this period, the mimetic musculature is usually so weakened that it cannot be restored. However, these cases are not hopeless: in older patients from about 75 years, static suspensions and muscle replacement operations can achieve considerable improvements in function and aesthetics.
Surgical procedures to restore the dynamics of the face can be performed simultaneously by rearranging still functioning muscle groups in the face. This can be used to successfully reconstruct partial functions of the facial expression of a completely or partially paralyzed half of the face.
With muscle rearrangements of certain muscle groups of the masticatory musculature, for example, functionally significant facial movements such as closing of the eyes and controlling the corner of the mouth to laugh and smile can be restored without impairing the masticatory function. The success of regained dynamic function and symmetry is already noticeable for the patient immediately after the operation.

Prior to surgery, this 85-year-old patient demonstrated massive asymmetry with a completely paralyzed right eye closure. In addition, a strongly drooping lower eyelid on the right and flaccid cheek tissue are visible. A loss of the facial nerve after tumor resection (acoustic neuroma surgery) led to chronic facial paralysis due to the loss of the entire mimetic musculature on the right side (left picture). Middle picture: Immediately after the reconstruction operation with a muscle rearrangement of the masticatory musculature (Gillies-McLaughlin or Labbe operation), the patient is able to close the right eye completely arbitrarily. Right picture: In addition to a clear gain in symmetry, the patient can produce an active smile after the operation and is strengthened in her social function.
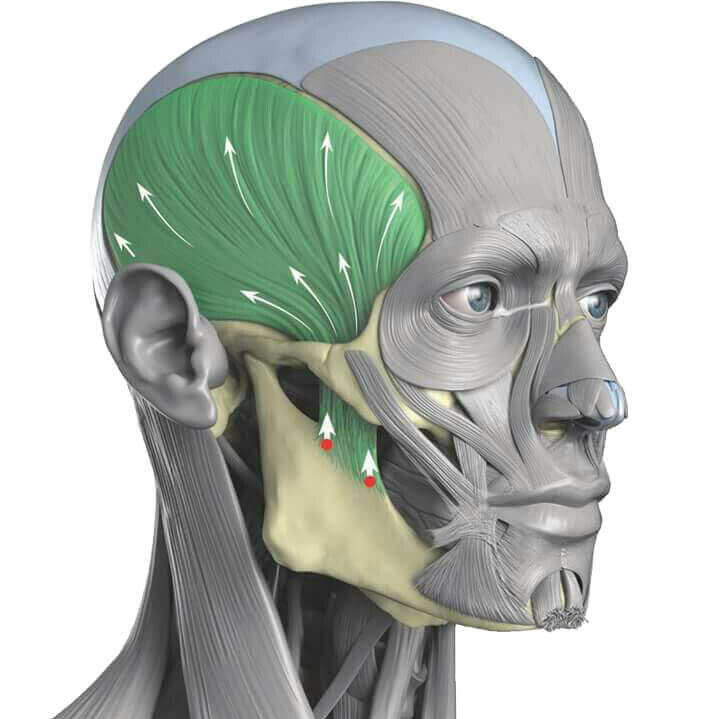
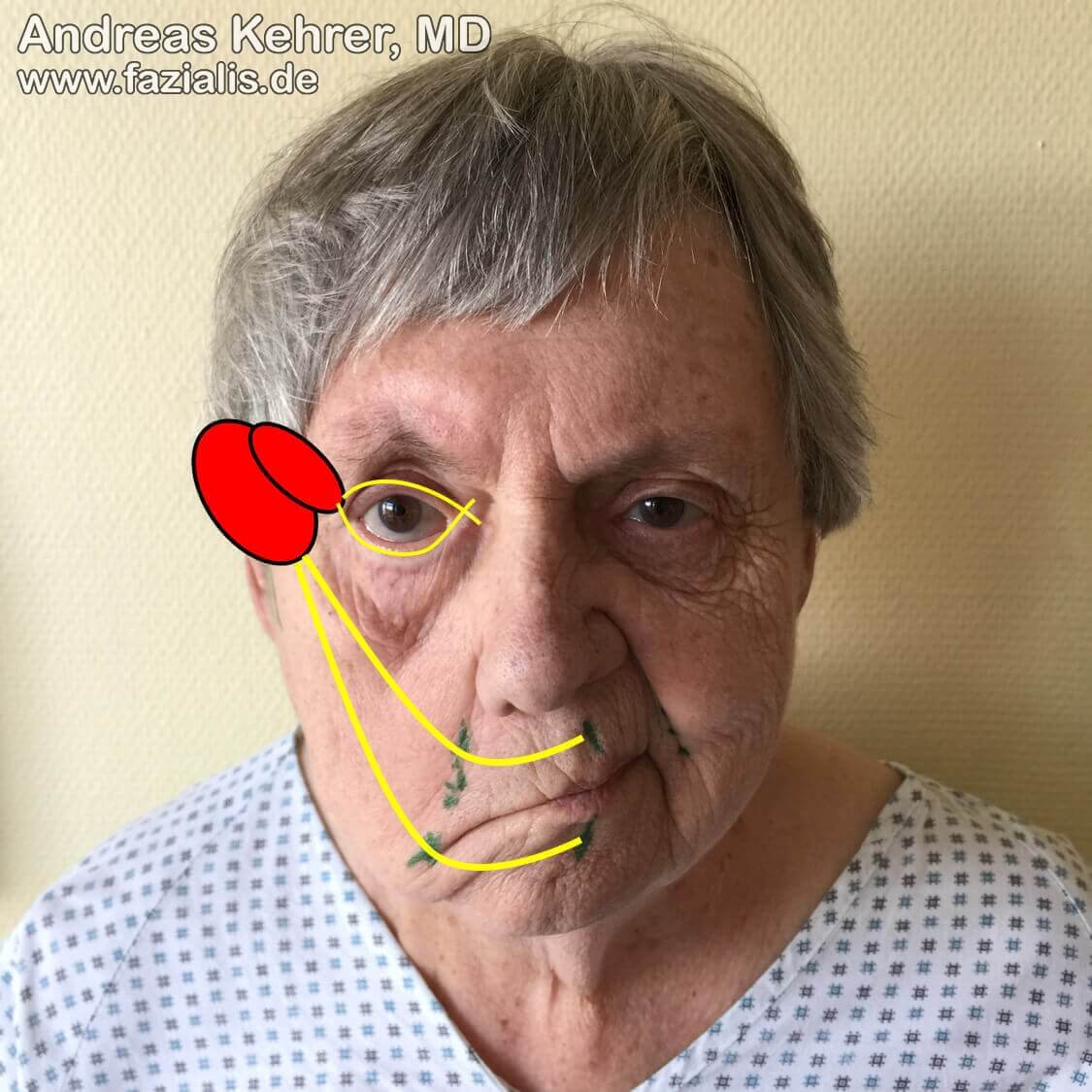
The temporal muscle is one of four essential masticatory muscles. It is a strong muscle. When chewing, as seen here in a good friend of the author, its contours are sometimes clearly visible. Parts of the Temporalis muscle are suitable for the restoration of an spontaneous eye closure (modified Gillies operation). The tendon of the entire muscle is used in the modified McLaughlin or Labbé operation to control the corner of the mouth. However, the patient does not have to expect reduced chewing function on this side, as the remaining chewing muscles compensate the function very well.
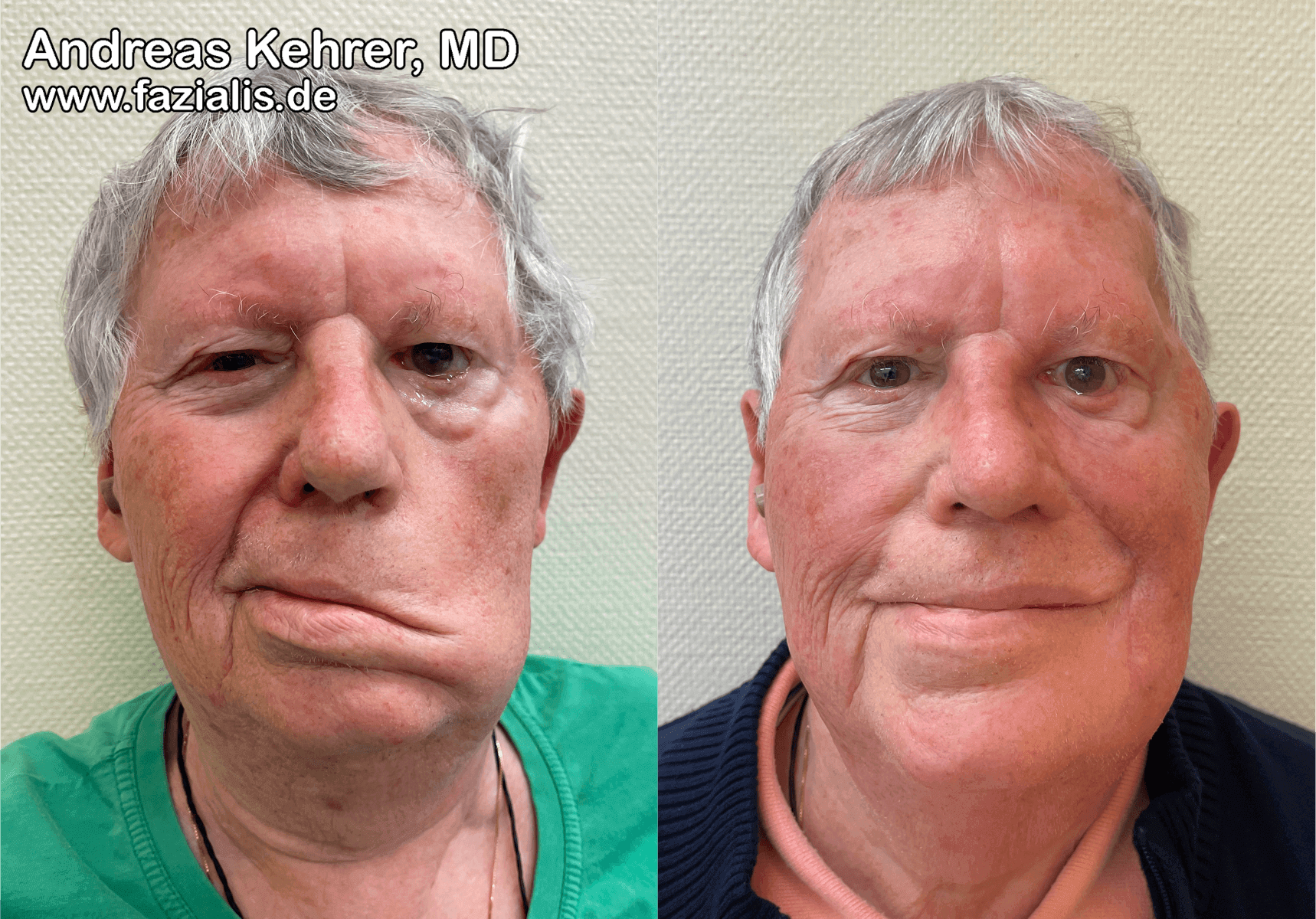
Long standing facial paralysis in elderly patients may also be successfully treated with temporalis muscle transfer. This 81-year-old patient complained of the typical symptoms of slackening of the temporalis muscle: frequent unintentional salivation with constant staining of his outerwear (lack of oral competence), difficulty in food processing during the chewing process (accidental biting of the oral mucosa and retention of food residues in the cheek pocket), and slurred speech (dysarthria). After surgical repositioning of the temporalis muscle (Labbé temporalis muscle transfer), both resting symmetry and dynamic function (facial expression) improved immensely. There are several positive effects at once: 1. significantly improved symmetry due to the recreation of the nasolabial fold and tightening of the corner of the mouth with a balancing of the lips at rest. 2. now active control of the corner of the mouth and the ability of a conscious smile/laugh. 3. no more accidental salivating and biting of the buccal mucosa 4. improvement in articulation with a clearer speech pattern due to less flaccid, "vibrating" cheek tissue and improved position of the corner of the mouth. 5. Significantly improved social function and psyche of the patient.
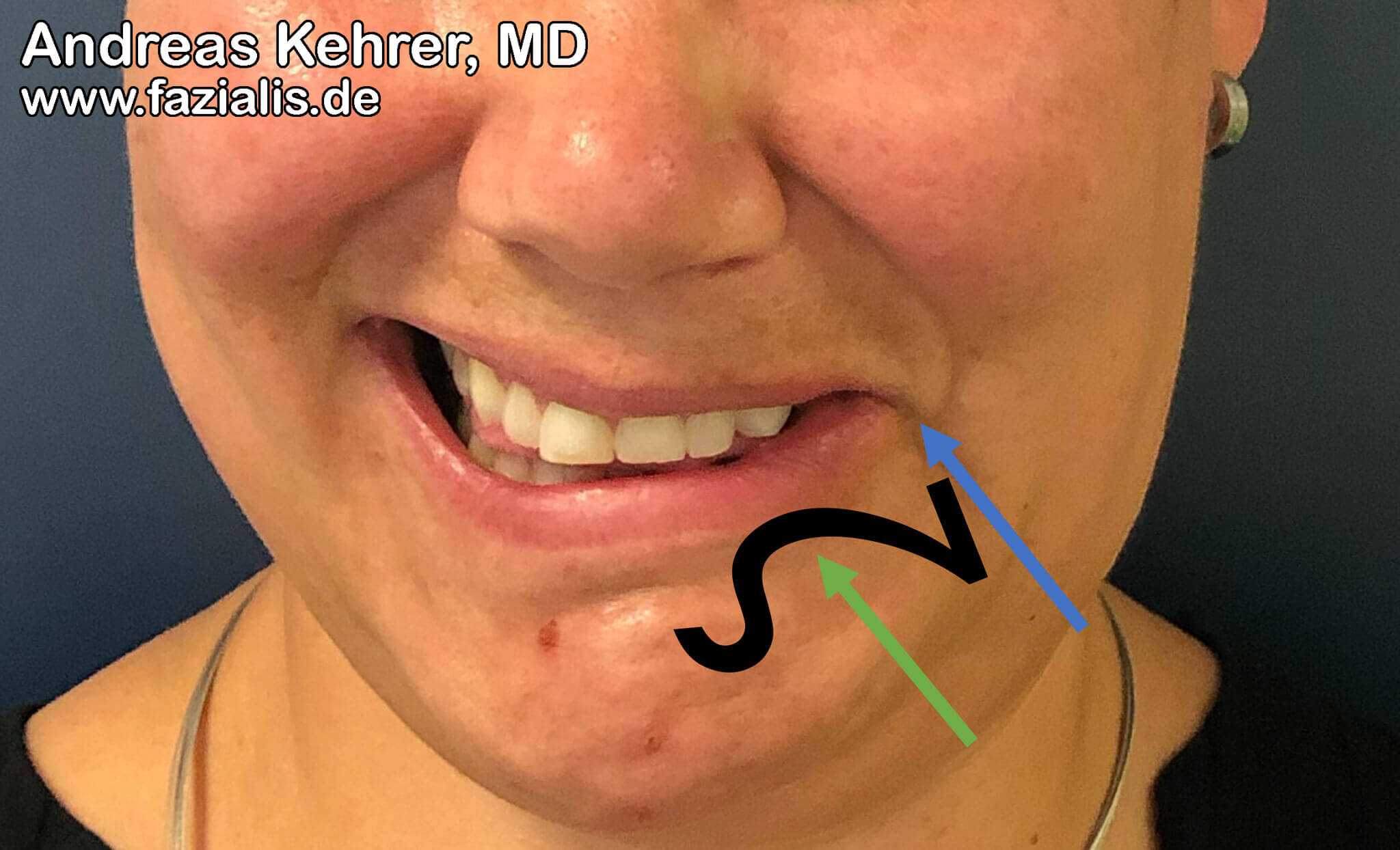
The mimic musculature, which is supplied by the facial nerve (Nervus facialis), significantly determines, among other things, the human smile. Accordingly, damage to the facial nerve is often accompanied by impaired smiling[1]. In this disease mechanism (pathomechanism), the depressor anguli oris muscle (DAO) is of particular importance. The DAO runs between the chin (tuberculum mentale) and a muscle node (modiolus)[2]. The modiolus is located approx. 1 cm above-laterally (superolaterally) of the corner of the mouth. While in healthy individuals the DAO is responsible for the emotional expression of anger and worry, for example, it can cause a misshapen smile in facial paresis patients. This occurs especially in cases of bark paresis, infections and lesions of the facial nerve in the temporal region[3-5]. Characteristic for a disturbed muscle function of the DAO is the so-called "zetadeformity" (see Fig. 1-2), which is based on an imbalance of the lip raising and lip lowering muscles. Another typical feature of "zeta deformity" is that a lower lip lowering muscle (M. depressor labii inferioris; DLI) is weakened, while the mouth angle lowering DAO is overactive and counteracts the pull of the mouth angle raising muscles during smiling. The limited functionality of the DLI in contrast to the DAO is based on its singular nervous supply[6]. In contrast, the DAO has a double nervous supply.
In order to restore a natural smile in such cases, PD Dr. med. Kehrer uses static and dynamic procedures - adapted to the respective patient. Static procedures include, for example, cutting the DAO (myectomy), interrupting the nerve supply to the DAO (neurectomy) or Botox therapy (botolinum toxin A). An additional therapy option is DAO muscle transfer, in which the position of the DAO is changed so that it now supports the natural smile[7]. Another option is modified selective neurectomy, in which smaller subbranches of the facial nerve are cut[8]. Thus, the respective problem areas can be tackled more specifically.
Dynamic therapy options include nerve transfer, muscle transfer and direct nerve supply to the muscles (direct neurotization)[9]. While a part of a thigh muscle (M. gracilis) is often useful for the replacement of the mouth angle elevating muscles, a part of the superficial neck muscles (Platysma), for example, is used for the purpose of DAO replacement[10].
The DAO also contributes to the formation of the so-called "marionette wrinkles", which run from the corner of the mouth towards the chin and can be treated e.g. with Botox (Botolinumtoxin A) or a transection of the DAO[11].

Function loss or inhibition of the depressor labil inferioris (DLI) cause a unilateral palsy of the lower lip with a high position. The mandibular teeth cannot be exposed arbitrarily (upper video). After a transfer of the depressor angulis oris (DAO) muscle as DLI replacement, the function of the lip depression on the right is largely restored (lower video)
Quellen:
[01] Krishnan Santha K, Joseph S, Latheef S, Narayanan S, Nair SM, Babu B, Sivadasan A, Shet SM, Pydi RV, Pati A, Samantaray SA. Dynamic smile reanimation in facial nerve palsy. J Korean Assoc Oral Maxillofac Surg. 2020 Apr 30;46(2):143-149. doi: 10.5125/jkaoms.2020.46.2.143. PMID: 32364354; PMCID: PMC7222615.
[02] Carey JC, Cohen MM Jr, Curry CJ, Devriendt K, Holmes LB, Verloes A. Elements of morphology: standard terminology for the lips, mouth, and oral region. Am J Med Genet A. 2009 Jan;149A(1):77-92. doi: 10.1002/ajmg.a.32602. PMID: 19125428.
[03] Azizzadeh B, Frisenda JL. Surgical Management of Postparalysis Facial Palsy and Synkinesis. Otolaryngol Clin North Am. 2018 Dec;51(6):1169-1178.
[04] Salles, A. G., da Costa, E. F., Ferreira, M. C., do Nascimento Remigio, A. F., Moraes, L. B., & Gemperli, R. Epidemiologic Overview of Synkinesis in 353 Patients with Longstanding Facial Paralysis under Treatment with Botulinum Toxin for 11 Years. Plastic and Reconstructive Surgery, 2015;136(6):1289–1298.
[05] Pepper J-P, Kim JC. Selective chemodenervation with botulinum toxin in facial nerve disorders. Operative Techniques in Otolaryngology-Head and Neck Surgery. 2012;23(4):297–305.
[06] Krag AE, Dumestre D, Hembd A, Glick S, Mohanty AJ, Rozen SM. Topographic and Neural Anatomy of the Depressor Anguli Oris Muscle and Implications for Treatment of Synkinetic Facial Paralysis. Plast Reconstr Surg. 2021 Feb 1;147(2):268e-278e.
[07] Klebuc M. Labio-mental Synkinetic Dysfunction (PowerPoint slides). Weill Cornell School of Medicine. 2020.
[08] Azizzadeh B, Irvine LE, Diels J, Slattery WH, Massry GG, Larian B, Riedler KL, Peng GL. Modified Selective Neurectomy for the Treatment of Post-Facial Paralysis Synkinesis. Plast Reconstr Surg. 2019 May;143(5):1483-1496.
[09] Bassilios Habre S, Googe BJ, Depew JB, Wallace RD, Konofaos P. Depressor Reanimation After Facial Nerve Paralysis. Ann Plast Surg. 2019 May;82(5):582-590.
[10] Manktelow RT, Tomat LR, Zuker RM, et al. Smile reconstruction in adults with free muscle transfer innervated by the masseter motor nerve: effectiveness and cerebral adaptation. Plast Reconstr Surg 2006;118(4):885–99.
[11] runeau S, Foletti JM, Holweck G, Laversanne S, Brignol L, Thiéry G. Traitement des plis d'amertume par section du depressor anguli oris: note technique [Marionette fold treatment by depressor anguli oris section: technical note]. Rev Stomatol Chir Maxillofac. 2012