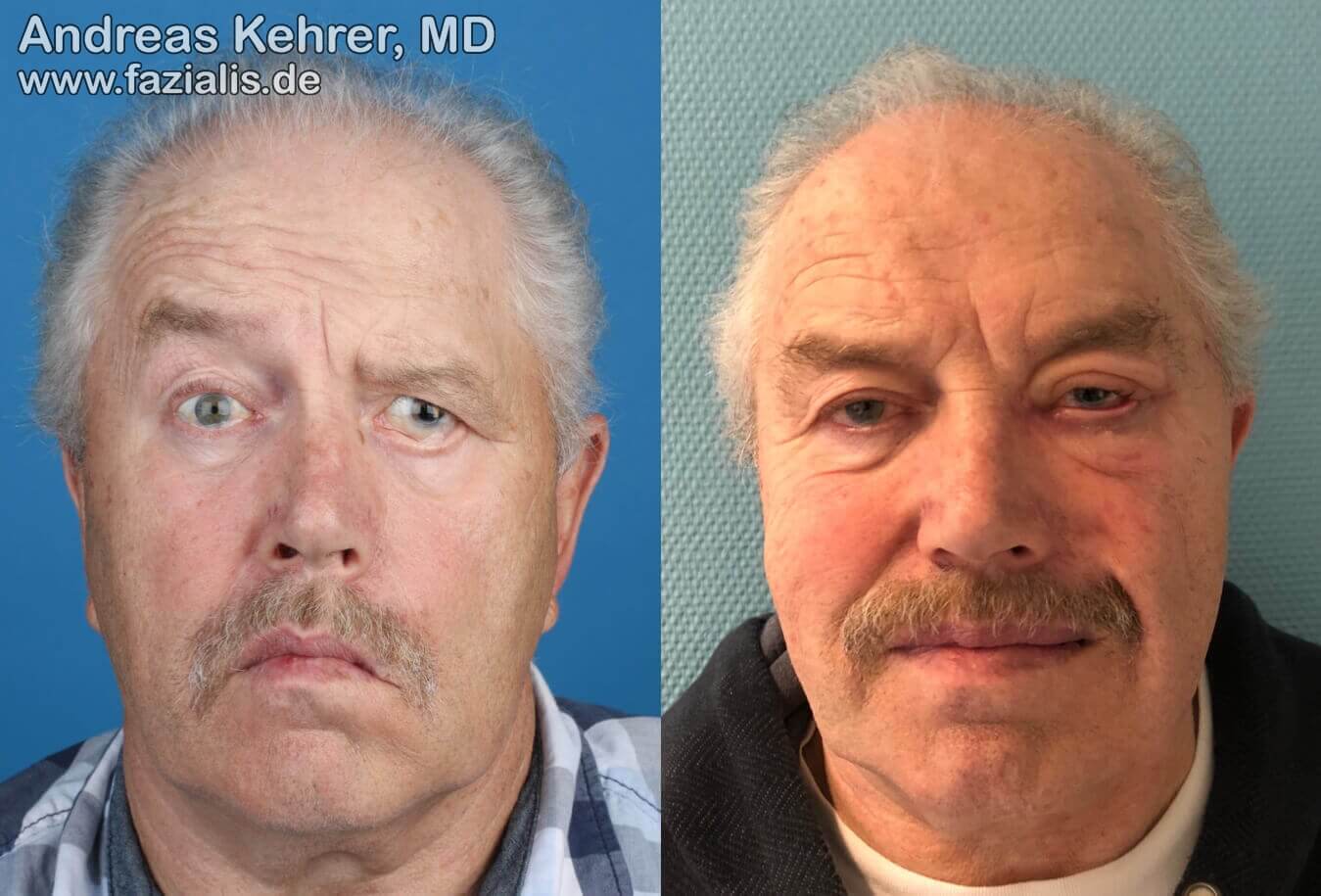
This 69-year-old patient suffered from spontaneous idiopathic facial paresis (Bell’s palsy) with a complete loss of the mimetic musculature of the left half of the face without signs of regression. Functionally, he suffered from a distinct eyebrow depression, a completely paralyzed orbicularis oculi (eye ring muscle) on the left with a massive hanging lower eyelid, and accompanying chronic conjunctivitis. Independent of the Bell's palsy, an eye injury occured on the left as a juvenile. The left picture also shows a more collapsed nostril on the left side (breathing through the nose is difficult) and a flaccid, hanging corner of the mouth, which led to oral incontinence (unintentional loss of liquid food). The right picture shows the situation of the patient after a two-stage reconstruction: in a first intervention, the patient received a combination of a static suspension procedure for the corner of the mouth and the nostrils and a free functional muscle transplantation into the left cheek region. The second procedure three months later was dedicated to the eye complex: lower lid reconstruction with autologous tissue and endoscopic brow lifting. The combination of both procedures leads both to an improvement of important functions (achievement of oral continence, improved nasal breathing, irritation-free eye without inflammation of the connective tissue, and improved speech due to firmer cheek tissue), as well as from the aesthetic appearance (improved symmetry in rest and facial expression). Postoperatively, a slight tissue swelling of the left eyelids is still present, which disappears after some time.