The classification into peripheral or central facial nerve paralysis is fundamental in medicine and important for understanding pathologies of the facial nerve. The distinction is of great clinical importance.
Central facial paralysis occurs when the source of paralysis lies in the brain. Due to the functional fiber arrangement and its course, central paralysis of the facial nerve is associated with preserved frown function and partially preserved lid closure. Strokes and brain tumors are common causes.
Peripheral facial paralysis occurs when the facial nerve is damaged in its course outside the brain. The extent of the paralysis depends on how far peripheral the damage is and can cause complete or incomplete facial paralysis.
Source: Modified by author: Patrick J. Lynch, Dr. C. Carl Jaffe, Cranial nerve IX 9 Bell's palsy, 12/23/2006, commons.wikimedia.org/wiki/File:Cranial_nerve_VII_bells_palsy.svg, accessed on 08/28/20, CC BY-SA 2.5. creativecommons.org/licenses/by-sa/2.5.
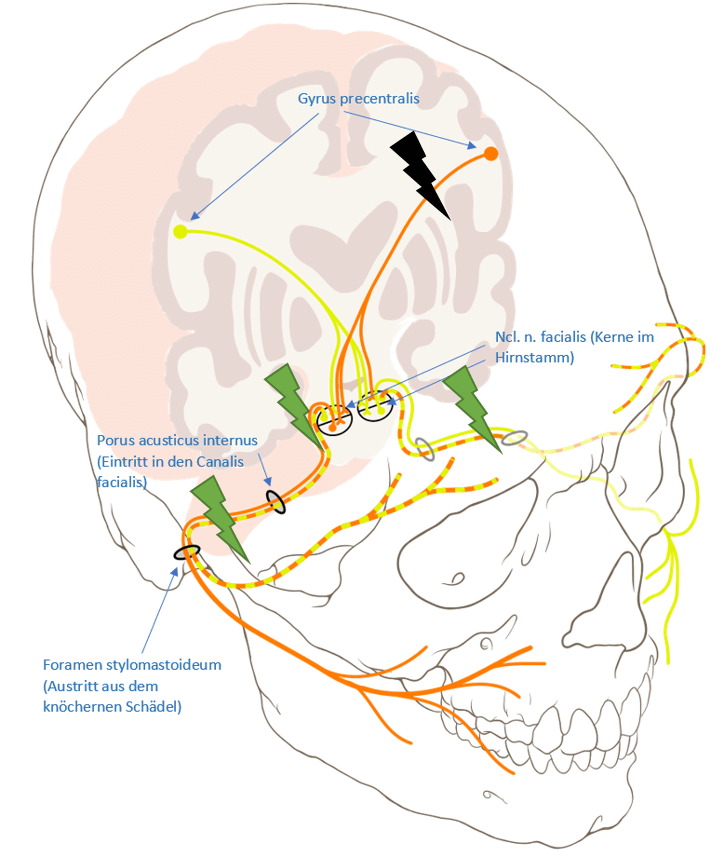
The graphic on the left should illustrate the lesion locations and the associated failure pattern.
Central: Facial paralysis is central when the cause of the paralysis is in the brain (black lightning). Due to the arrangement of the fibers (crossing of the forehead branches; interconnection of the orange and yellow fibers in the cranial nerve cores), central paralysis is accompanied by preserved frown function and partially preserved lid closure (the forehead branch is controlled by yellow and orange), as this is still controlled by the intact other half of the brain. As can be seen in the diagram, damage in the left hemisphere of the brain is accompanied by loss of the right side’s function (note crossing of the pathways in the cranial nerve nuclei). Strokes and brain tumors are common causes.
Peripheral: If the nerve lesion is located further downstream from the cranial nerve nucleus a peripheral paralysis results (green flashes). The damage is localized on the side of the failure symptoms, because the crossover already takes place in the brain. Therefore, in contrast to central paralysis, the forehead area is usually also affected by the paralysis. The extent of the paralysis depends on how far peripheral the damage is. Depending on the location of the damage (e.g. in the main nerve stem area in the temporal bone or only in a peripheral nerve branch in the midface region), complete or incomplete facial paresis may be present. The topographic evaluation of the lesion is further complicated by the fact that, for example, a complete lesion of all nerve fibres (axons) versus only a partial lesion of nerve fibres (e.g. 25%) in one nerve cross-section may be present. The exchange of nerve fibers by “anastomoses” (cross-linking) of nerve branches and sub-branches complicates exact anatomical determination of the lesion on the basis of clinical criteria.