Reshaping of a nasolabial fold
The Nasolabial fold ("nose-lip-furrow"; from lat. nasus "nose" and labium "lip") is a soft-tissue-deepening which exists that on both sides of the face between the corners of the mouth and the nasal ala. This brings a special characteristic to the the face. The shape, depth, and length of the nasolabial fold are determined by the facial muscles, the different extent of the subcutaneous fatty tissue present and the age[1].
Nasolabial folds are of major importance for symmetry. If they are missing on one side, as is often the case with flaccid facial paralysis, the result is a rather noticeable disturbance of the facial symmetry. An effaced nasolabial fold is completely missing. It can be restored by various plastic surgery techniques. Ideally, it can be restored "naturally" by introducing new muscles (muscle transplantation or muscle rearrangement) through the newly gained underlying muscle activity. If this is not possible, it can be reconstructed with precisely inserted static suspension procedures. Frequently, an additional incision is made in the skin using a special suturing technique.
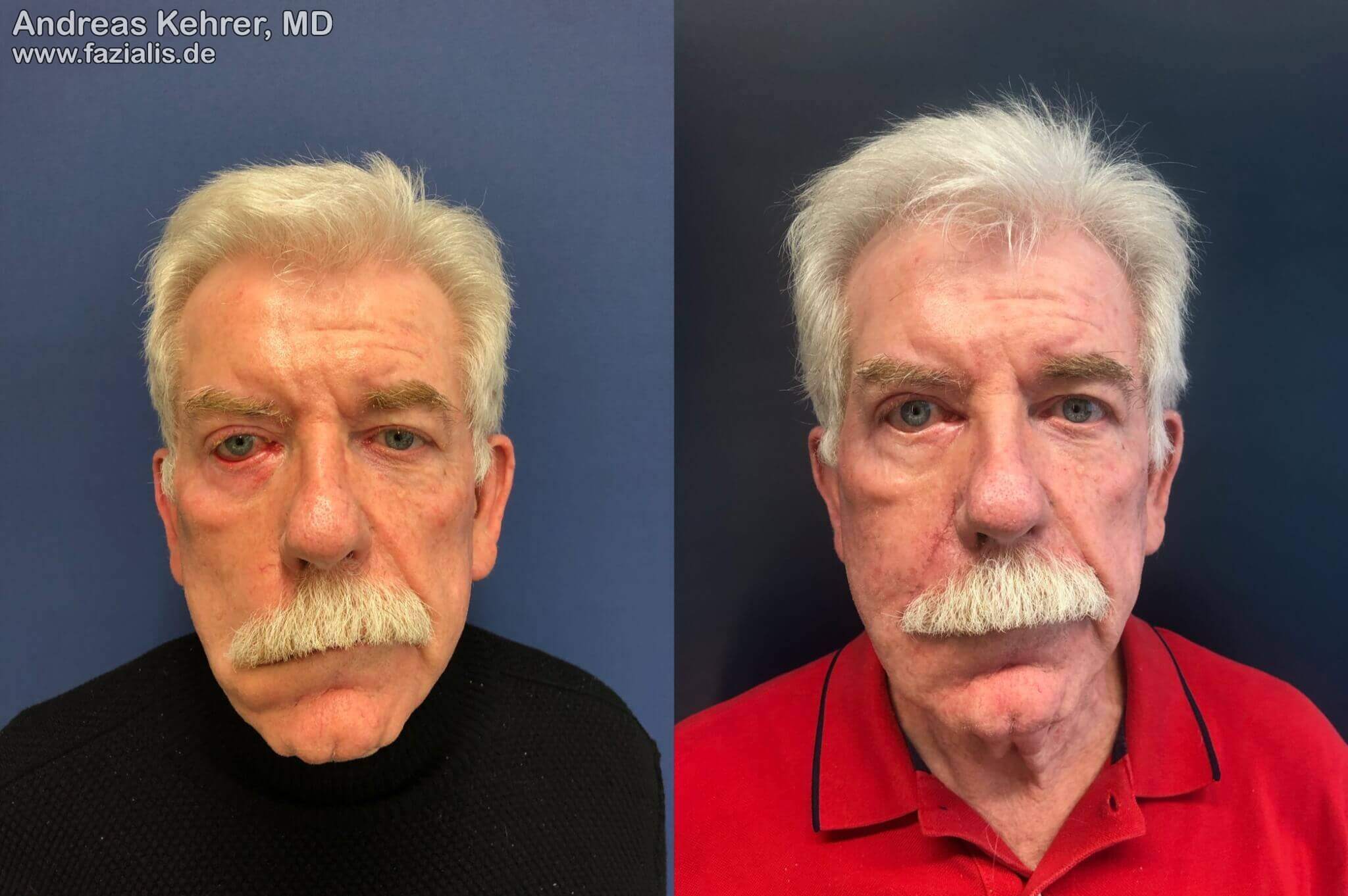
This 71-year-old patient with chronic facial paralysis received a temporal transfer (muscle replacement plastic) together with a reshaping of the right nasolabial fold. The resting symmetry has been significantly improved by repositioning of the right corner of the mouth and the reshaping of the nasolabial fold.

This patient presented 25 years after a a temporal bone fracture with facial nerve palsy. All prior treatments had taught her that she had to come to terms with her paralysis, as there were no treatment options. She complained of a clear restriction of her visual field, regular conjunctivitis, significant oral incontinence, and blurred speech. Furthermore, she would inadvertently bite the mucous membrane of the flaccid inner cheek repeatedly and during the chewing process the food remained regularly in the "cheek pocket", which she would have to pull out with her finger. A three-stage reconstruction scheme was performed, which included a Labbe operation (Temporalis transfer procedure) with new formation of a nasolabial fold, insertion of a platinum weight into the upper lid in a hidden position, correction of the lower lid ectropion, correction of the tarsorraphy of the outer eyelids performed elsewhere, and eyebrow lift. All symptoms were either corrected or significantly improved. The patient reported that drinking was much easier for her because she could control the corner of her mouth much better. She now dared to do this again in company, as she no longer constantly dirtied her outerwear. At the moment, we are planning a fat transfer to get her lips even more "watertight".
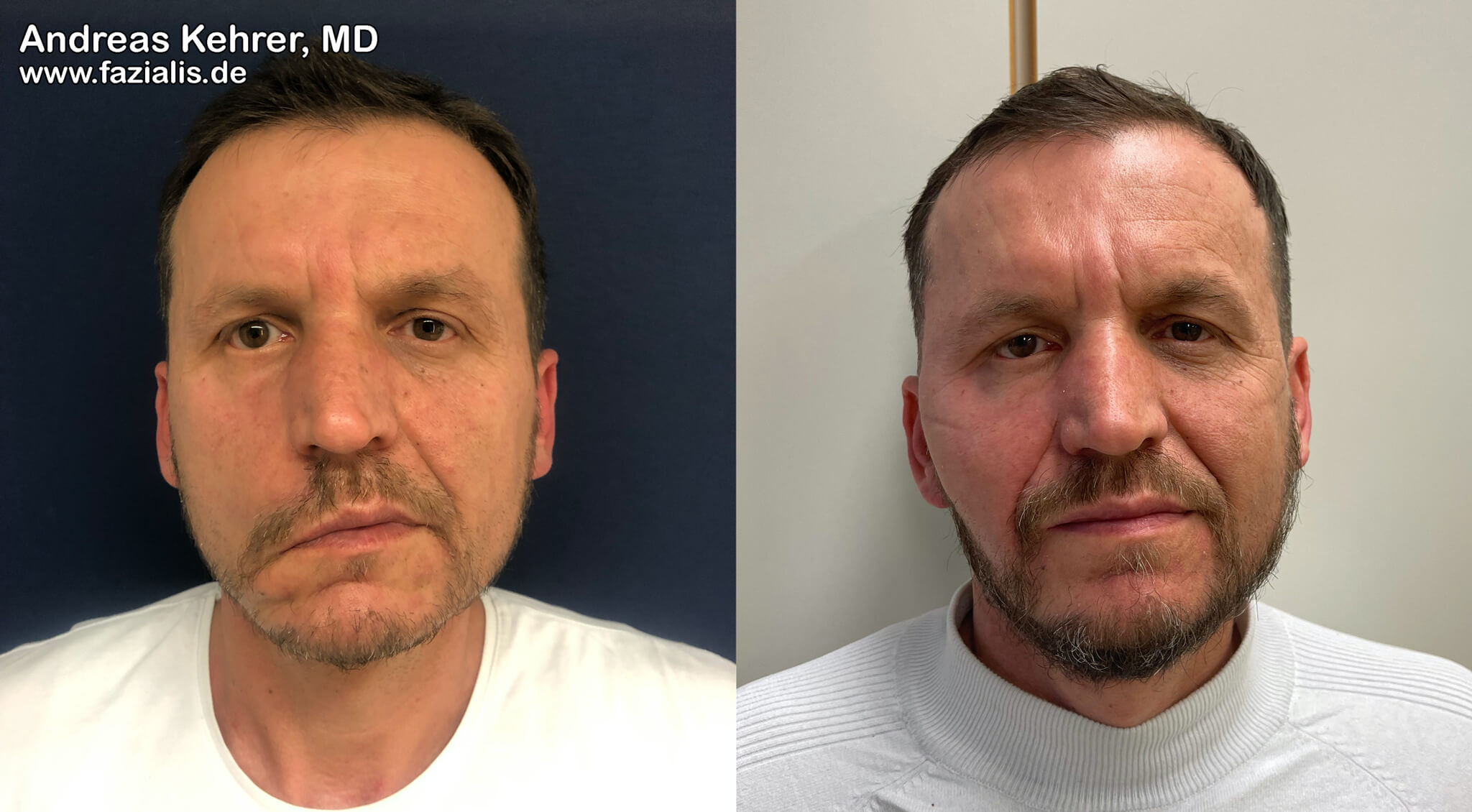
Before and after surgical recreation of the nasolabial fold, higher positioning of the corner of the mouth and free muscle transplantation as a combination procedure of static and dynamic restoration in a 45-year-old patient. It becomes clear how much symmetry is already conveyed at rest (without facial expression) by the uniform configuration of the natural smile line.