Paralysis of the facial nerve is also accompanied by symptoms in the mouth area. Muscle weakness of the mouth region may be a sign. For example, a drooping corner of the mouth and food residue remaining in the cheek pocket of the affected side may be evident.[1] Oral incontinence may also occur, i.e. the inability to keep fluids in the mouth. Furthermore, taste disorders may occur in the front two-thirds of the tongue, since these are not nerved by the ninth cranial nerve (N. glossopharyngeus) like the rear third of the tongue, but by a branch of the facial nerve (Chorda tympani). Reduced sensitivity to taste is mainly found in young patients with Bell's Palsy.[2] In addition, facial nerve palsy can also result in dry mouth (xerostomia). The earlier an insufficient moistening of the mouth occurs, the more severe the paresis appears and the less chance there is of the symptoms subsiding.[3] Facial nerve palsy can also be followed by atrophy of the orbicular muscle (M. orbicualris oris). Interestingly, branches of the facial nerve sometimes counteract the healthy opposite side of this atrophy.[4] But fat grafting can also help here. Another oral symptom of facial nerve palsy is trismus.[5] The Melkersson-Rosenthal syndrome, which is classically characterized by the triad of facial nerve palsy, lip swelling, and tongue furrows (tongue fissures), must be differentiated.[6] In addition to the known scoring systems (here, please link to Scores), lip length, i.e. the intercommissural distance (ICD), can be used to make statements about the function of the perioral muscles around the mouth.[7]

Figure 1
Mimic musculature: 1: M. levator labii superioris aleque nasi (upper lip and nasal wing lifter), 2: M. levator labii superioris (corner of mouth lifter), 3: M. zygomaticus minor (small cheek bone muscle), 4: M. zygomaticus major (large cheekbone muscle), 5: risorius muscle (laughing muscle), 6: buccinator muscle (cheek muscle), 7: depressor anguli oris muscle (mouth angle counterbore), 8: depressor labii inferioris muscle (lower lip counterbore)
In this 3D learning model from our friends at ANATOMYNEXT (www.anatomynext.com), the layered structure of the mimic musculature becomes clear. Thus, the mouth angle counterbore (M. depressor anguli oris), the eye ring muscle (M. orbicularis oculi) and the superficial part of the small cheekbone muscle (M. zygomaticus minor) form the most superficial level. This is followed by the deep portion of the M. zygomaticus minor, the large cheekbone muscle (M. zygomaticus major), the laughing muscle (M. risorius), the neck skin muscle (Platysma) and the upper lip and nasal wing lifter (M. levator labii superioris alaeque nasi). The third layer is composed of the mouth ring muscle (M. orbicularis oris) and the upper lip lifter (M. levator labii superioris). The deep layer contains the cheek muscle (M. buccinator), the corner of the mouth lifter (M. levator anguli oris) and the chin muscle (M. mentalis). Interestingly, no gender-specific differences in length, width and thickness of the mimic muscles can be detected. The 3D learning model was created by our friends from ANATOMYNEXT (www.anatomynext.com), who enrich our site with their excellent 2D and 3D teaching models.
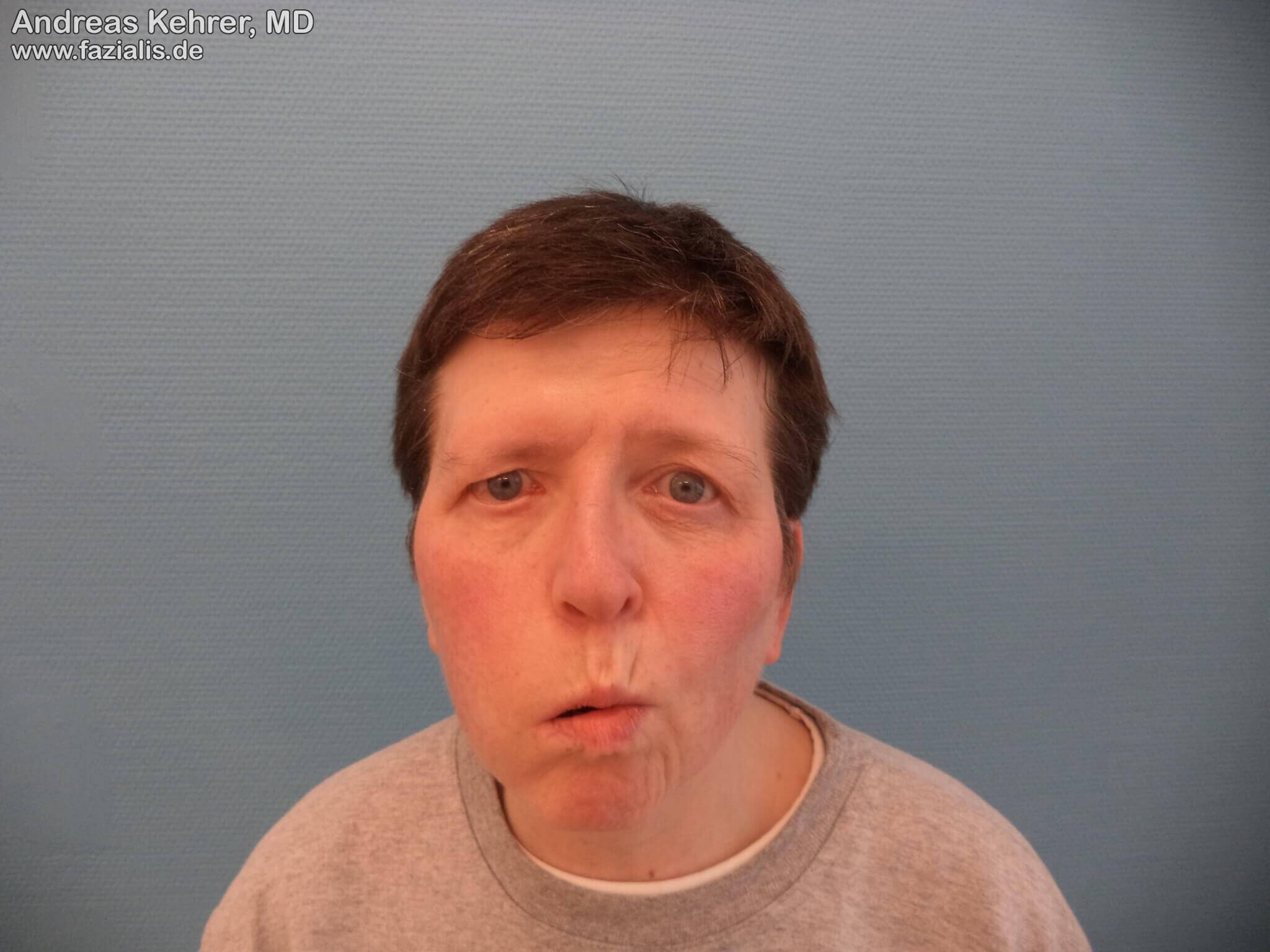
Figure 2
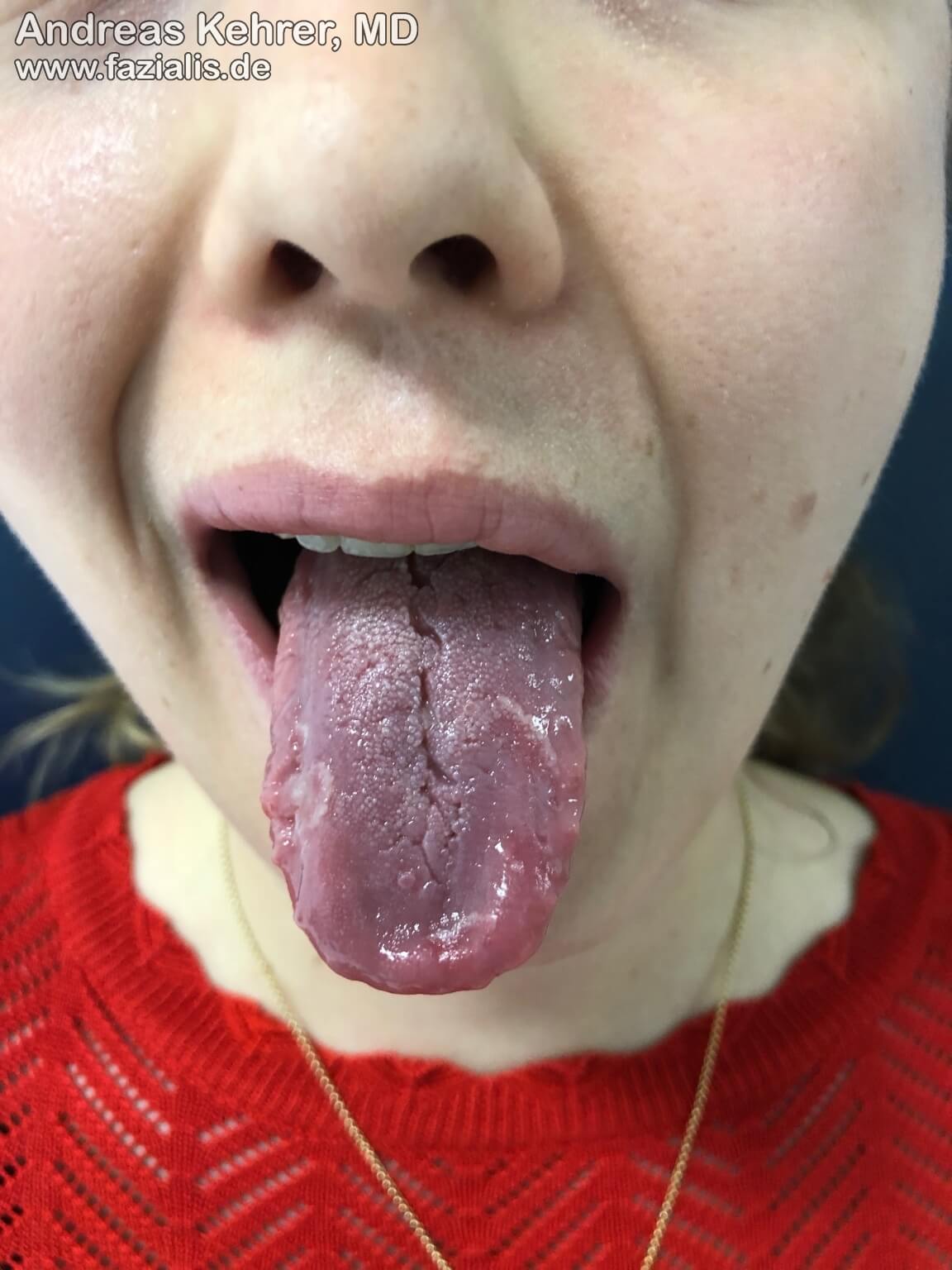
When the patient is asked to "inflate the cheeks" and at the same time keep the air in the oral cavity, this fails on the right side. The paralyzed cheek muscles on the right side are responsible for this, as is the clearly weakened ring muscle around the mouth region. A firm pressing together of the lips is not possible on the right side compared to the left side. Muscle atrophy is already clearly apparent by the lack of muscle volume in the area of the right upper and lower lip
In this 3D learning model from our friends at ANATOMYNEXT (www.anatomynext.com) you can visualize the course of the cheek muscle (M. buccinator). This muscle originates from a bone ridge (Crista buccinatoria) in the area of the Proc. coronoideus of the lower jaw. From there, it moves in the direction of the Modiolus, a muscle node located approximately 1 cm laterally of the corner of the mouth. The failure of the M. buccinator may, for example, be the cause of food resi-due remaining in the cheek pocket. The 3D learning model was created by our friends at ANATOMYNEXT (www.anatomynext.com), who enrich our site with their outstanding 2D and 3D teaching models.
This 54-year-old lady with complete facial paralysis on the right side gives an impressive demonstration of the symptoms of paralysis in the mouth area. The loss of the ring muscle and the cheek muscles leads to blurred speech. Liquid food is difficult or impossible to retain in the oral cavity. The muscles controlling the mouth angle and the upper lip lifters have failed. When a smile is attempted, there is a clear asymmetry.
Attempting to laugh with "teeth showing" increases the asymmetry. The component of the missing upper lip lifting musculature comes to the fore even more clearly. At the same time, the dependence of the involuntary blinking reflex in the right eye on the facial nerve can be clearly observed; this is missing in comparison to the non-paralyzed opposite side.
Sources:
[1] Somasundara D, Sullivan F. Management of Bell's palsy. Aust Prescr. 2017 Jun;40(3):94-97. doi: 10.18773/austprescr.2017.030. Epub 2017 Jun 1. PMID: 28798513; PMCID: PMC5478391.
[2] Park JM, Kim MG, Jung J, Kim SS, Jung AR, Kim SH, Yeo SG. Effect of Age and Severity of Facial Palsy on Taste Thresholds in Bell's Palsy Patients. J Audiol Otol. 2017 Apr;21(1):16-21. doi: 10.7874/jao.2017.21.1.16. Epub 2017 Mar 30. PMID: 28417103; PMCID: PMC5392006.
[3] De Seta D, Mancini P et al. Bell's palsy: symptoms preceding and accompanying the facial paresis. ScientificWorldJournal. 2014;2014:801971. doi: 10.1155/2014/801971. Epub 2014 Nov 27. PMID: 25544960; PMCID: PMC4270115.
[4] Biglioli F, Allevi F, Battista VM, Colombo V, Pedrazzoli M, Rabbiosi D. Lipofilling of the atrophied lip in facial palsy patients. Minerva Stomatol. 2014 Mar;63(3):69-75. English, Italian. PMID: 24632798.
[5] Klobucar, R., Kingsmill, V., Venables, V., Bisase, B., & Nduka, C. (2012). A dental perspective of facial palsy. Faculty Dental Journal, 3(4), 202–207.doi:10.1308/204268512x13466824724634.
[6] Ang KL, Jones NS. Melkersson-Rosenthal syndrome. J Laryngol Otol. 2002;116:386–8.
[7] Jansen, C., Devriese, P. P., Jennekens, F. G. I., & Wijnne, H. J. A. (1991). Lip-length and Snout Indices in Bell’s Palsy:A Comparison with the House Grading System. Acta Oto-Laryngologica, 111(6), 1065–1069.doi:10.3109/00016489109100757.